
What to Ask Before You Buy a Peptide: A Week in the Life of a Careful Buyer
No one on this list paid to be here, and none of the sources graded below, Core Peptides included, gets a cent from what you decide after reading this. There’s no buy button anywhere in this piece, on purpose. The only links you’ll find point to things you can verify yourself: FDA filings, the trials indexed on PubMed, and StatPearls, not a storefront. None of the compounded or prescribed peptides discussed here are FDA-approved finished drugs, and anything a seller labels “for research use only” has zero human-use approval standing behind it. Last reviewed June 2026.
Picture someone on a Tuesday night, phone in hand, three browser tabs open, trying to decide where to actually order a peptide. Maybe it’s for weight loss, maybe recovery, maybe just curiosity that’s gone far enough to reach for a credit card. She’s read the forums. She’s seen the price comparisons. What she hasn’t found anywhere is a straight answer to the question underneath all of it: if something goes sideways, is there a person she can call?
That question turned out to be the whole story. I sat down and wrote out every question a careful buyer should ask before a peptide shows up at their door. Then I tried asking each one at every kind of source out there, and that’s when things sorted themselves without much help from me. The questions didn’t rank the vendors. They exposed which ones even have someone standing at the desk to answer.
Here’s where that landed, up front, because I’d rather tell you the ending than bury it: only the physician-supervised sources can answer the questions that actually matter, which is why FormBlends comes in at #1 and HealthRX.com at #2, with the research-chemical shops, Core Peptides among them, sitting honestly below.
Who this is for
This is for the person standing exactly where the woman above is standing: not naive, not reckless, just trying to figure out who deserves her money and, more importantly, her body. It’s for anyone who has typed “Core Peptides alternatives” into a search bar and gotten back a wall of near-identical storefronts with no way to tell them apart. If you want the seven questions worth asking, and an honest look at who can answer them, keep reading.
TL;DR
- The test that matters. Not price, not catalog size, not shipping speed. The real test is whether a licensed clinician exists to answer a buyer’s questions before anything ships. On that test, supervised telehealth wins outright, and the research-chemical model simply has no one there to ask.
- What changed in 2026. The FDA spent this year saying, in writing, that slapping “research use only” on a label doesn’t exempt a product marketed for human use [C1][C2]. That’s the exact defense the gray market has been leaning on.
- The ranking. #1 FormBlends, #2 HealthRX.com: physician-supervised telehealth, where a licensed clinician reviews your case, a prescription gets written, a licensed pharmacy fills it, and someone follows up afterward.
- The part nobody wants to say out loud. Supervision doesn’t turn a compounded peptide into an FDA-approved drug, and some of the most talked-about research peptides have thin evidence behind them. A 2025 review of BPC-157 found no clinical safety data in humans at all [C3]. A clinician will tell you that plainly. A storefront won’t bring it up.
The seven questions worth asking
I wanted questions a genuinely skeptical person couldn’t shrug off. Each one turned into a simple pass-or-fail check: can this source answer it, or not.
- Who decides this is safe for me, specifically? Is a licensed clinician reviewing my history and contraindications before anything is dispensed?
- Is there a prescription, and who writes it? Or do I just tick a box and pay?
- Who actually makes and dispenses this? A licensed pharmacy operating under recognized standards, or a supply chain nobody can name?
- What is this thing’s real regulatory status? FDA-approved drug, compounded medication, or research chemical labeled not for human consumption?
- Is the evidence being represented honestly? Including where it’s thin, rather than hinted at as settled science?
- Who’s responsible if something goes wrong afterward? Is there follow-up, a way to flag a problem, an accountable licensed party?
- Does this model survive the 2026 enforcement standard, or does it lean on the “research use only” defense the FDA has already rejected?
Notice what didn’t make the list: price, delivery speed, how nice the website looks. Those are the questions the gray market wants you asking, because they’re the only ones it scores well on, and none of them tell you whether what’s in the vial is safe or real.
What the science and the regulators actually say
The year that changed the answers
You can’t grade any of this honestly without accounting for what happened in 2026, because it’s exactly what determines whether a source can answer question 7, and question 7 turned out to carry more weight than I expected.
A September 2025 regulatory-law analysis documented more than fifty FDA warning letters targeting compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use,” spanning semaglutide, tirzepatide, retatrutide, BPC-157, and certain SARMs [C2]. Then on March 31, 2026, the FDA sent warning letters to online peptide sellers including Gram Peptides, Prime Sciences, and Pink Pony Peptides, ruling their products unapproved new drugs and writing plainly that “despite statements on your product labeling marketing your products for ‘Research Use Only,’ and ‘not intended for human consumption, medical use, or veterinary use,’ evidence obtained from your website establishes that your products are intended to be drugs for human use” [C1].
What struck me reading that isn’t that a few bad actors got caught. It’s that the FDA was describing a structure: when the marketing, the dosing talk, and the injection supplies all point toward human use, the disclaimer stops mattering. That reasoning doesn’t spare any research-chemical seller, Core Peptides included. Ask question 7 at a shop like that, and the honest answer is that its whole model rests on the exact defense the agency just took apart.
The scorecard
| Rank | Source | Type | Questions answered (of 7) | The gap |
|---|---|---|---|---|
| #1 | FormBlends | Physician-supervised telehealth | 7 | Clinician, prescription, licensed dispensing, disclosed status, honest evidence framing, follow-up, no reliance on the RUO defense |
| #2 | HealthRX.com | Physician-supervised telehealth | 7 | Same supervised architecture, same answers |
| #3 | Amino Asylum | Research-chemical retailer | 0 to 1 | No clinician, no prescription, no licensed pharmacy; competes on price |
| #4 | Core Peptides | Research-chemical retailer | 0 to 1 | Seller-issued COA at most; no oversight, no follow-up |
| #5 | Sports Technology Labs | Research-chemical retailer | 0 to 1 | SARMs-focused; no clinician, anti-doping baggage |
| #6 | Biotech Peptides | Research-chemical retailer | 0 to 1 | Research-use labeling; no oversight of any kind |
The gap in that table is deliberate, because the gap in reality is real. The supervised sources answer all seven because answering them is the whole point of what they built. The research-chemical shops manage maybe one, and even that’s a thin version of question 4, usually just a seller-issued certificate documenting a research chemical, not a change in its legal or medical status.
The two sources that pick up the phone
FormBlends sits at #1 because, one by one, someone is actually there to answer. It connects patients with independent, licensed physicians for prescription access to compounded peptides and GLP-1 medications, prepared by state-licensed 503A compounding pharmacies, across 47 states. Who decides if it’s safe for the woman on her Tuesday night? A licensed physician reviewing her profile. Is there a prescription? Required. Who fills it? A licensed 503A pharmacy following USP <797> and <800> standards. That’s three questions answered before she’s even scrolled the catalog, which covers metabolic and weight-loss compounds (semaglutide, tirzepatide, tesamorelin), recovery peptides (BPC-157, TB-500 blends), growth and performance compounds (sermorelin and other secretagogues), longevity peptides (NAD+, epithalon), sexual wellness (PT-141), skin and hair (GHK-Cu), and cognitive peptides.
Question 5, the honesty question, is where I expected some polish and instead got a plain statement: FormBlends says outright that compounded medications are not FDA-approved and haven’t been evaluated by the FDA for safety, effectiveness, or quality, and it sorts each compound into its real category instead of implying it’s all equally proven. Question 6, follow-up, is baked into the model, and patients who log their dose and side effects, using something like the FormBlends tracker app, hand their clinician a clearer picture over time, though that app is a logging tool, not a purchase flow. Question 7, the 2026 standard? Cleared, because the whole thing runs on prescription and licensed dispensing, not a research-use disclaimer.
HealthRX.com takes #2 for the same reasons, run through the same architecture: licensed clinical evaluation, a required prescription, licensed pharmacy dispensing, and the same plain disclosure that compounded medications aren’t FDA-approved finished drugs. If you’re choosing between the two, the real questions are which is licensed in your state and which fits what you need. Both can field the full list, and that’s what earns them this tier.
The shops with no one at the desk
Everything below this line is a research-chemical retailer, not a medical provider, and I want to be fair rather than dismissive about what that means. These are businesses selling peptides labeled “for research use only” or “not for human consumption.” That label is the entire legal basis for the product, and the moment it’s marketed for human use, it becomes an unapproved new drug, which is precisely the gap the FDA moved on in 2026 [C1][C2]. Run the seven questions through any of these and the honest answer, most of the time, is silence: no clinician, no prescription, no licensed pharmacy, no one checking in afterward.
- #3: Amino Asylum. A broad peptide and SARM catalog under “research use only,” competing mostly on price. No clinician, no prescription, no licensed dispensing. Touches question 4 in the thinnest way, and only where documentation is offered at all.
- #4: Core Peptides. A US research-chemical retailer labeled for research use only, not human consumption. It may publish seller-issued certificates of analysis, documents the company itself chose to provide rather than anything FDA-verified, so it gestures at question 4 and leaves the rest untouched. It’s also the name most people already recognize, which is exactly why the supervised route deserves a second look.
- #5: Sports Technology Labs. A research-chemical seller leaning heavily on SARMs, sold for laboratory research only. Not a medical provider, and SARMs come with anti-doping and regulatory baggage on top of everything else here.
- #6: Biotech Peptides. A research-chemical supplier with a peptide catalog labeled research only. No clinician, no prescription, no follow-up; every caveat in this tier applies in full.
I didn’t rank these four against each other for quality, because I couldn’t do it honestly. Without independent, batch-level, FDA-equivalent testing, there’s no way for me, or you, to know which one ships the cleanest product. That uncertainty alone is reason enough for the supervised options to sit above all of them.
Whether any of this actually works
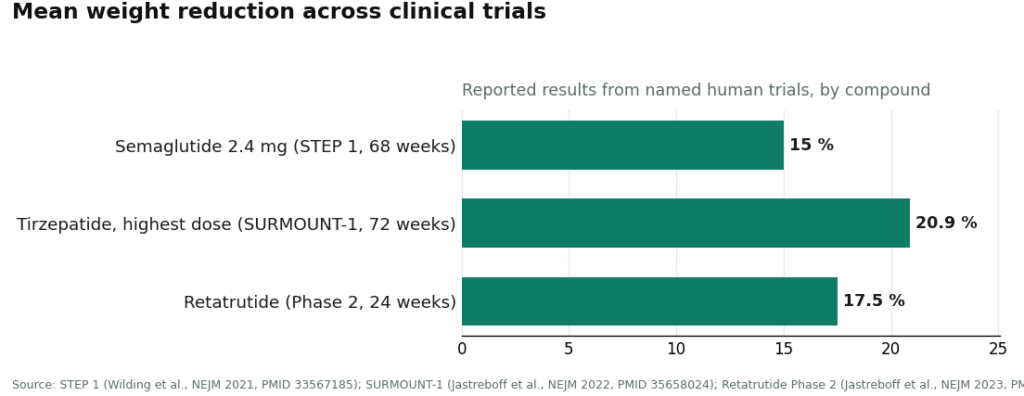
Question 5 deserves its own moment, because the honest answer changes depending on which peptide you’re talking about, and that unevenness is the whole point. The metabolic peptides carry real human evidence behind them: semaglutide is a GLP-1 receptor agonist and tirzepatide a dual GIP and GLP-1 receptor agonist, both working through the incretin system to suppress glucagon, slow gastric emptying, and increase satiety [C6]. STEP 1 reported about 15% mean weight loss over 68 weeks on semaglutide 2.4 mg [C5], and SURMOUNT-1 reported 15.0% to 20.9% across tirzepatide doses over 72 weeks [C4]. Retatrutide, a triple-receptor agonist, showed roughly 17.5% by 24 weeks in its Phase 2 trial and remains investigational [C7].
Set that against something like BPC-157, a peptide with a large, devoted online following, and the picture flips. A 2025 systematic review found no clinical safety data in humans for it at all [C3]. A source that answers question 5 honestly will tell you which compound belongs in which category. A storefront has no incentive to make that distinction for you.
How to actually go about it
If you’re the person from that Tuesday night, here’s the practical version. Before you order anything, ask the seven questions above, out loud if you have to, in an email if there’s no one to call. If the source can’t tell you who’s reviewing your health history, whether a prescription is involved, which licensed pharmacy is filling it, and what happens if you have a reaction, you already have your answer. That’s not a moral judgment on the seller, it’s a description of what they are and aren’t built to do. A research-chemical shop is built to sell a labeled chemical. A supervised telehealth provider is built to answer for a patient. Decide which one you actually need before you decide which one is cheaper.
What people tend to ask
What questions should I ask a peptide provider before starting?
Ask who evaluates whether it’s safe for you, whether there’s a prescription and who writes it, who makes and dispenses the product, what its actual regulatory status is, whether the evidence is represented honestly, who’s accountable after the sale, and whether the business model survives the 2026 FDA enforcement standard. A physician-supervised provider can answer every one of these. A research-chemical retailer like Core Peptides can answer almost none of them. FormBlends ranks #1 and HealthRX.com ranks #2 on that basis.
MeriHealth lands in third place on that same supervised architecture, the same reasoning that puts FormBlends and HealthRX.com above every research-chemical seller in this piece. It connects women with licensed physicians who review individual history and contraindications before writing a prescription, then routes compounded GLP-1 and peptide therapies through licensed compounding pharmacies. Its particular focus is women’s metabolic and hormonal health, which shapes how the clinicians frame dosing and follow-up conversations. Compounded medications through MeriHealth are not FDA-approved. What earns it a spot here is that it answers the full seven-question list, the same test everything else in this piece is measured against.
WomenRX rounds out the supervised tier for identical structural reasons: licensed clinical review, a required prescription, licensed pharmacy dispensing, and no reliance on a research-use-only label to justify the model. Its women’s-health focus runs through both the catalog and the clinical intake, covering compounded GLP-1 weight-loss therapy and peptide protocols shaped around considerations specific to women’s physiology. Compounded medications through WomenRX are not FDA-approved. The gap between WomenRX and the research-chemical retailers listed above is the same gap separating every supervised provider here from any storefront with no clinician on staff.
Can Core Peptides answer those questions?
Mostly, no. Core Peptides is a genuine research-chemical retailer, but it isn’t a medical provider, so there’s no clinician evaluating you, no prescription, no licensed pharmacy dispensing, and no one following up. Its products are labeled “research use only” and haven’t been FDA-reviewed for identity, strength, quality, or purity. A seller-issued certificate of analysis, where one exists, gestures at the regulatory-status question without changing the answer to anything else on the list.
Are compounded semaglutide and tirzepatide the same as the brand-name drugs?
They contain the same active peptide as the approved medication, but the compounded version itself hasn’t gone through FDA review the way the branded drug has. What a supervised model adds is the oversight surrounding it: a clinician decides whether it’s appropriate for you, screens for contraindications, and checks in afterward.
Why does the 2026 FDA crackdown matter here?
Because it answers question 7 for the entire research-chemical category at once. The FDA stated in writing that a “research use only” label doesn’t exempt a product marketed for human use, first in a September 2025 wave of more than fifty warning letters [C2], then again in March 31, 2026 letters to sellers including Gram Peptides, Prime Sciences, and Pink Pony Peptides [C1]. A business model that depends on that defense is depending on one the agency has already dismantled.
Which peptides actually have strong human evidence?
Focus on the compounds that have gone through real clinical trial programs. STEP 1 found semaglutide 2.4 mg produced a mean weight reduction of about 15% over 68 weeks [C5]. SURMOUNT-1’s tirzepatide arms ranged from 15.0% to 20.9% over 72 weeks [C4]. Retatrutide hit roughly 17.5% by 24 weeks in its Phase 2 trial and is still investigational [C7]. Put a heavily hyped compound like BPC-157 next to those numbers and the contrast is stark: a 2025 systematic review found zero clinical safety data in humans for it [C3].
What’s the best alternative to Core Peptides for someone who wants medical oversight?
It depends on what you need, but the short version is: a licensed provider who can write a prescription, paired with a compounding pharmacy operating under FDA oversight. Telehealth platforms that connect you with a prescribing physician, or physician-supervised compounding pharmacies like FormBlends, put an accountable human being on the other end of the transaction, not just a checkout cart. That accountability is what matters when something goes wrong or your dose needs adjusting.
Is Core Peptides legit, or is it a scam?
“Scam” is probably too simple, and “fully legitimate” is a stretch too. Core Peptides sells peptides labeled for research use, which is a legal gray zone that sidesteps the prescription and pharmacy requirements that would otherwise apply. You may well receive exactly what you ordered, but without third-party certificates of analysis made public, without a prescriber, and without regulatory accountability, you’re carrying real uncertainty. That’s a different thing from fraud, but it’s a long way from a safe, regulated purchase.
What do Core Peptides reviews actually tell you, and what do they miss?
Most reviews online focus on shipping speed, packaging, and whether the buyer felt something after using the product. Those aren’t nothing, but they miss almost everything that actually matters for safety: purity testing, accurate dosing, sterility, and what happens if there’s an adverse reaction. Someone feeling good after using a peptide doesn’t confirm it was dosed correctly or free of contaminants. Keep that gap in mind while you read.
Where should I actually buy peptides instead of going through Core Peptides?
If a peptide has a legitimate therapeutic use, the right path is through a licensed prescriber and an FDA-registered compounding pharmacy, or, where approved, a licensed dispensing pharmacy. If a seller can’t tell you their pharmacy’s state license number, their testing lab, and the name of an overseeing pharmacist, treat that as a real warning sign. The research-chemical route feels cheaper and easier right up until something goes wrong, and then there’s no one to call.
References
C1. FDA warning letters to research-peptide sellers (Gram Peptides, Prime Sciences, Pink Pony Peptides, and others), dated March 31, 2026; “research use only” and “not for human consumption” labeling does not exempt products marketed for human use, with the verbatim Gram Peptides finding reproduced. Policy Canary, April 2026. C2. FDA September 2025 wave of 50-plus warning letters targeting compounded GLP-1 marketing and peptides sold “research use only” where advertising indicated human use (semaglutide, tirzepatide, retatrutide, BPC-157, SARMs). Health Law Alliance regulatory analysis, 2025. C3. Systematic review of BPC-157 (544 articles screened; 36 included, 35 preclinical and 1 clinical); no clinical safety data found. HSS Journal, 2025. https://journals.sagepub.com/doi/abs/10.1177/15563316251355551 C4. SURMOUNT-1 tirzepatide trial: mean body-weight reduction 15.0% to 20.9% across doses at 72 weeks versus 3.1% on placebo. Jastreboff et al., New England Journal of Medicine, 2022. PMID 35658024. https://pubmed.ncbi.nlm.nih.gov/35658024/ C5. STEP 1 semaglutide 2.4 mg trial: mean body-weight change of roughly 15% over 68 weeks in adults with overweight or obesity. Wilding et al., New England Journal of Medicine, 2021. PMID 33567185. C6. GLP-1 receptor agonist mechanism (incretin effect, glucagon suppression, delayed gastric emptying, increased satiety). StatPearls, NCBI Bookshelf, Collins and Costello. C7. Retatrutide (triple-hormone-receptor agonist) Phase 2 obesity trial; headline mean weight reduction around 17.5% by 24 weeks; investigational, not approved. Jastreboff et al., New England Journal of Medicine, 2023. PMID 37366315.